Much of the vaccine debate is presented as a "black and white" or "us vs. them" fight, it's really a many shades of gray, no, a many hues of all colors affair. There's one aspect about one battle that epitomizes all this.
While I appreciate a tightly written story, one with story lines nicely woven together, this isn't one of them. If I'm lucky, it might pull together down at the conclusion.
Among the (pick one or two)
groups, people are
that SARS-CoV-2 vaccines are associated with an elevated risk of
in the days after vaccination. I will focus on just myocarditis, most of what I say here will apply elsewhere.
Myo (muscle) card (heart) itis (inflammation) is inflammation of the heart, the muscle that moves blood throughout the body. It works best when it's not inflamed because inflammation generally means the heart is damaged or will soon be. Its prevalence is claimed to be "The European Medicines Agency said that, depending on the source, the incidence of myocarditis and pericarditis ranges from 1 to 10 in 100,000 people a year." There's also pericarditis, inflammation of the pericaridum around the heart, and myopericarditis. One paper says "Hereafter, myocarditis is used to refer to myocarditis, pericarditis, or myopericarditis." Good idea, except others refer to simply carditis which makes more sense to me.
After the initial glowing reports from Pfizer/BioNTech's vaccine and its 95% reduction in infection rate in the test group, several things have gradually changed, perhaps I'll expand on that some day, but probably not. The major concern was that some people experienced a serious allergic response, hence the 15 minute period of hanging around after the vaccination. (Personal experience - after my first dose of the Pfizer/BioNTech vaccine I noticed an increase in salivation. I attributed that to reading a Chinese take out menu as I was going to call in an order after my 15 minutes were up.)
I think a few reports of myocarditis emerged early on, they increased after May 10, 2021 when Pfizer gained authorization for administering it to children aged 12 years and older. This issue has grown into a key symbol in some circles that claim (pick one):
A small group of people came up with (pick one):
Aspiration? I'll get back to that, but first....
In the following sections, I refer to several papers. They generally use the research names of the vaccines involved, in part for precision, in part because it's shorter. Here's the decoding key for companies, technology and names. Not all of these are reports I link to.
Pfizer/BioNTech (mRNA): BNT162b2 or Comirnaty (version given final FDA approval)
Moderna (mRNA): mRNA-1273
J&J/Jannsen (adenovirus): Ad26.COV2.S
AstraZeneca (adenovirus): ChAdOx1-S
Some of the reports of incidence of myocarditis (these figures may include pericarditis and myocarditis) follow. All numbers are per 100,000 people, a 'X" suffix means times the historical rate, which might be that 1 to 10 mentioned above.
5.4X of all recipients? An editorial in the BMJ (British Medical Journal says 2.7. 13.60X of males age 16-19 and the second dose. An editorial in the BMJ says 7 but doesn't specify which dose.
I can't make sense of:
The rate ratio 30 days after the second vaccine dose in fully vaccinated recipients, as compared with unvaccinated persons, was 2.35 (95% CI, 1.10 to 5.02); the rate ratio was again highest in male recipients between the ages of 16 and 19 years (8.96; 95% CI, 4.50 to 17.83), with a ratio of 1 in 6637.
They conclude:
The incidence of myocarditis, although low, increased after the receipt of the BNT162b2 vaccine, particularly after the second dose among young male recipients. The clinical presentation of myocarditis after vaccination was usually mild.
BNT162b2: 1.4 overall, 1.3 female, 1.5 male, 1.6 age 12-39.
Moderna: 4.2 overall, 2.0 female, 6.3 male, 5.7 age 12-39.
These figures are lower than Israel's, and while various ideas are considered to explain the difference, they didn't consider whether aspiration (there's that word again) was used.
This is a preliminary report based on submissions to VAERS (Vaccine Adverse Event Reporting System), a voluntary system. Many cases are missed, but also many reports will not meet the strict diagnostic criteria for myocarditis, however it is good for finding things that need further study.
Males after second dose: 6.28 age 12-17, 5.05 age 18-24, 0.24 age 30+
Females after second dose: 0.42 females age 12-29, 0.10 older females
Myocarditis reporting rates were 40.6 cases per million second doses of mRNA COVID-19 vaccines administered to males aged 12-29 years and 2.4 per million second doses administered to males aged ≥30 years; reporting rates among females in these age groups were 4.2 and 1.0 per million second doses, respectively. The highest reporting rates were among males aged 12-17 years and those aged 18-24 years (62.8 and 50.5 reported myocarditis cases per million second doses of mRNA COVID-19 vaccine administered, respectively).
BNT162b2: 18.5 age 12-17: 3.4 after first dose, 21.2 after second.
males age 12-17: 5.6 after first dose, 37.3 after second.
This data sound much cleaner than the US data. It's also three months later, after the alarm had been sounded.
This is a population cohort study in Hong Kong that monitored adverse events following immunization through a pharmacovigilance system for COVID-19 vaccines. All adolescents aged between 12 and 17 years following Comirnaty vaccination were monitored under the COVID-19 vaccine Adverse Event Response and Evaluation Programme. The clinical characteristics and overall incidence of acute myocarditis/pericarditis in adolescents following Comirnaty vaccination were analysed.
As these findings trickled in, people began to worry about what was going on and how to deal with it.
The [CDC] Advisory Committee on Immunization Practices presented data showing that even among young men there were relatively few myocarditis cases given the total number of covid-19 cases prevented. Among adolescent boys ages 12 to 17 the researchers estimated that, for every one million second dose vaccinations, 5700 covid-19 cases, 215 hospital admissions, 71 intensive care unit admissions, and two deaths would be prevented. Against this there might be an estimated 56 to 69 cases of myocarditis.
Prasad believes that the US decision is wrong and that it is better to play it safe. "Vaccination always serves two purposes," he said, "firstly to benefit the person who gets it and secondly to benefit others. We are willing to do things for the second purpose but not if they are a net harm to individuals." He thinks that the US should suspend all vaccination in children under 18 and give only one dose of vaccine to men under 25.
This is a power point presentation mostly on myocarditis reports in VAERS (Vaccine Adverse Event Reporting System) and VSD (Vaccine Safety Datalink). Useful to show how myocarditis was reported in the two datasets. This is closely related to the US study above.
This is an article apparently in response to another article that says the CDC data is too low. The complaints about this paper could be applied to the CDC's paper as they both use VAERS:
However, the study has been widely criticised for mining data from an inappropriate source to deliver an antivaccine message, despite warnings against such data uses.
A preprint was modified to include a defense by the authors of the criticised report.
From my reading of the CDC report, the VAERS data was useful to identify a this rare concern and matches pretty well the better controlled VSD. It has data on 12 million persons per year from nine healthcare organizations.
This looks at the current information about myocarditis and gives most attention to the low rate in Denmark compared to other countries. The author makes no reference to aspiration (we're almost there).
I may look into this further, but a big point in all this goes back to Pfizer's phase 3 trial that led to the first Emergency Use Authorization. The trial included 21,720 people, age 16 and older, who received the vaccine. One of them had a myocardial infarction, none had myocarditis. The age range is one with a low incidence of myocarditis so it's not surprising that it was not detected in the vaccinated group. I don't know the size of the trial that led to the 2021 May 21 EUA for people age 12-15. Cases were noted soon afterwards, so that affirms we found it reasonably promptly with the mass vaccination process.
Overall, the incidence of myocarditis is low. Only when people realized that young males were at the highest risk did it warrant closer study.
On the other hand, the low incidence in Denmark was observed, but no research uncovered why.
There are two ways to perform an intramuscluar (IM) injection. In the past it was stick the syringe into the muscle, pull back on the plunger a bit to verify the needle isn't in a vein, then inject. More recently, the "aspiration" phase has been dropped. As best as people can tell, the WHO said it wasn't necessary for a pediatric vaccine and caused more pain. Somehow this has been adopted as standard practice in many countries for all vaccines. My three injections were the typical plunge, inject, withdraw sequence.
This has caught the attention of Dr. John Campbell (PhD in nursing). When the Delta variant arose, I started following his near-daily YouTube posts. He had several posts about aspiration, and added several more since. His very reasonable concern is that if the vaccine is injected intravenously (IV), it will quickly flow to the heart, then lungs, back to the heart, and then to the rest of the body. Should the vaccine nanoparticles attach to the heart muscle, it will start producing the spike protein and hence attract the attention of the immune system which will trigger inflammation (-itis). In support of that hypothesis, he and readers have accumulated these observations:
Some of his older readers had no idea aspiration had been discontinued.
Aspiration in the past may have prevented these sorts of issues. Perhaps it's part of
the reason why researchers never considered aspiration as an explanation for the low
myocarditis rate in Denmark.
Some of them reported cases where aspiration has disclosed the needle was in a blood vessel.
Overall, it's a rare occurrence, but it's an existence proof that lets us assume vaccines
are occasionally injected into veins.
Some people with serious reactions to mRNA vaccines reported a metallic taste seconds
after the injection.
No one has an explanation for this except for injection into a vein.
Adolescent males are most commonly affected.
It's unclear why - I suspect scrawny kids may have thin enough skin and muscle to allow
the needle to reach a vein between the deltoid muscle and bone.
Germany has recently instituted aspiration to their policy, they may be the only new adopter.
Campbell has started a campaign to restore aspiration to the process and is frustrated that public health people are not following up. People who have asked for aspiration have often been told that's no longer necessary.
One of his videos is an interview with Niels Høiby, a microbiologist in Denmark, who became convinced that some early cases of severe reactions to a Pfizer/BioNTech were due to unintentional IV injection. After seeing Denmark's Crown Prince was injected without aspiration, he convinced Denmark's medical establishment to restore aspiration, and did so early in the vaccination campaign. He and Campbell are convinced that this is the reason behind Denmark's low rate of myocarditis. I agree.
More research should be done, but given the long history that aspiration has not shown problems (outside of painful injections), I'm disappointed it hasn't been adopted everywhere, especially in the USA, where I live.
One animal study that strongly supports the IV injection hypothesis was done in Hong Kong. Mice were injected with one of four options: mRNA vaccine intramuscularly, mRNA vaccine intravenously, or saline solution, either IM or IV. A two dose regimen was followed to mimic the human protocol. Mice were sacrificed and dissected at different times within the protocol.
The most striking finding was that white patches appeared a day or two after the second dose, here are the hearts of IV saline, IV vaccine, and IM vaccines from mice two days after the second dose:
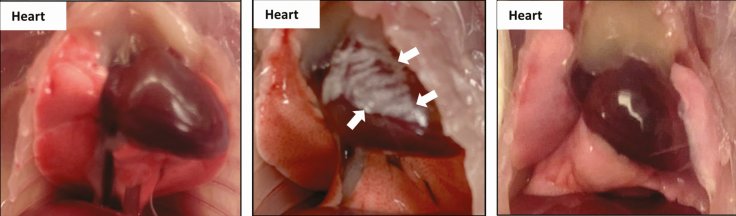
N.B. The paper refers to this photo with "Autopsy at 1-2 dpi [1 or 2 days post injection] showed white patches over the visceral pericardium in 37.5% (1 dpi, n = 8) to 38.5% (2 dpi, n = 13) of the IV vaccine group but none in the IM vaccine or NS control groups." However, a subsequent table with 2 days post injection data reports white patches were observed in 33.3% (n = 9) after the second IV dose and 16.7% (n = 6) after the second IM dose. Perhaps a simpler summary is that 8 of 21 mice had patches 2 days after an IV injection, while 1 of 18 mice had patches 2 days an IM injection.
While this page focuses on myocarditis issues, there are also concerns about rare cases of blood clots after the adenovirus based vaccines. However, there are similar anecdotal, retrospective, and mouse studies that are very similar to the myocarditis side effects. In fact, Professor Høiby's attention was drawn to the aspiration issue by an American patient who wound up in the ICU after vaccination. Problems in multiple organs suggested to him something systemic caused by IV injection.
My impetus for writing this page is that many people I associate with on FaceBook and elsewhere have latched on to the risk of myocarditis as a reason to not get vaccinated. I deem the risk low since it wasn't caught in phase 3 trials. When I put forth the aspiration hypothesis it either gets ignored, or people agree it deserves more study, but in the meantime they still resist/oppose getting vaccinated. I cannot fathom why people fear more the risk of myocarditis or thrombosis and discount the risks of even a mild case of Covid-19. We know what Covid-19 can do to the heart!
I hope this winds up being worth the time it took to write. Given that the Omicron surge is almost spent and nothing is in the wings, I doubt many people will read this. Ah well, some truckers are wasting much more time to driving the country to protest vaccinations, err, mandates. [Update, 2022 July 15] I wrote that in March 2022. Boy was I wrong. We're up to Omicron's BA5 subtype which is pretty good at evading vaccinations and even past infections.
[Update 2022 Nov 2] I just joined a phase 3 study of a Pfizer mRNA influenza vaccine. There was a 50-50% chance of getting either the standard vaccine or the mRNA study vaccine. Much to my amazement, the person who administered the shot aspirated it. Even more to my amazement, I didn't see her do it. When I mentioned aspiration, she showed me the slight motion that is all it takes with the syringes she had.
I will be sharing this page with my doctor's office any pretty much any medical site to ask them to include aspiration in all IM injections, I hope you do so too.
Written 2022 Mar 3, text last updated 2022 Nov 3.